

As crowds of people waited in line for health services, I asked patients questions about where they got their drinking water, their living situations, and I was always told to ask women if they were pregnant or could possibly be pregnant. I found that many of these girls were afraid to admit they were pregnant, and would deny it until there was proof in a pregnancy test. This was Bocas Del Toro, Panama. The towering waterfalls and trees of vibrant green could not cover up the complex realities of an indigenous community that suffers in the hands of the viruses and diseases that have roamed this earth for centuries. In an age of modern technology and healthcare, why is it that not everyone can have access to a healthy life? This was one of the many questions that could not escape my mind during my time volunteering for the Floating Doctors, a healthcare organization that provides health clinics to indigenous communities in Panama. I worked beside professional doctors, but I felt out of place. Was it moral for me, an eighteen year old, to ask such prying questions—even in the interest of improving their health?
Gazing into the eyes of each of the patients, I could see the impacts of their community and how it affected each person differently. Their stories were told on their faces and carried on their shoulders. I met people who were proud of their life’s accomplishments and the work they had done raising a family, starting a local business, helping clean up trash on the streets, or even just being proud that they stepped outside of their family unit for medical help from strangers. I was surrounded by the faces of those who have been abandoned by society; those who can only turn to their community to feel safe. As I sat at the make-shift clinic, atop a large square of cement, under the shade of metal roofing sheets, those people were finally being accepted. They were treated like real human beings, whose lives mattered. But there is only so much one can do. The most riveting instance I encountered was a fourteen year old who denied her pregnancy and STDs even after doctors had found both those results in her tests. I witnessed her world shatter. I reflected on how terrifying it was for a young girl, four years my junior, to either become a mother, or to make the decision to risk her life with an illegal abortion. She was begging the doctors for an abortion, crying, screaming, doing anything she could to rid herself of the future she saw ahead of her. Throughout that week the doctors I worked with told stories of young girls who were pregnant, or women who had been raped by other members of their community. I witnessed young, pregnant women coming to the clinic hand-in-hand with men who were old enough to be their grandfathers, calling them their husbands. This observation is not coming from a judgment of their culture, but it comes out of a concern for the health and well-being of these women who have no reproductive education or access to healthcare.
Now, I must also mention the beautiful experiences I had, and the wonderful people I met. I will never forget a young girl I spent hours with one day. During my lunch break at the clinic, a little girl about ten years old bravely asked other student volunteers to help her with her homework. Unfortunately, none of them spoke enough Spanish to understand her, so she finally asked me, and I was overjoyed to help her. She had a worksheet of English homework; after doing my best to teach English in a language I am not fully fluent in, this girl did not leave my side. As I continued to help the doctors I was working with, she held onto my arm. It confused me at first. Why did she feel so connected to someone who did not speak her language, and whom she had only known for a few hours? It was at that moment that I had realized the importance of making connections with people. Yes, “people” is broad, but it should be. There are so many people in this world, and one small moment, one small connection can change someone’s life forever. When she grabbed my arm, I could feel an immediate connection, for I could feel and see the true impact of my being there. I believe that these clinics are about human connection: giving hope to individuals and communities who may have lost it. I cannot deny that providing Depo shots and Albendazol helps their health and well-being too, but there is a much deeper impact of human connection with each visit. Although this essay is meant to examine why the Ngäbe Buglé do not have adequate access to healthcare and how that affects the gender dynamics, I must make it extremely clear that you must not dehumanize and ‘other’ these people. There is a beautiful connection between every human being in this world, and with time, you will feel and see exactly what I felt in that moment.
My goal is to connect the beauty of those in our species as a whole: homo sapiens. Many of our fellow homo sapiens live in dehumanizing conditions, and those who do not must lift their veil of ignorance to see the world clearly and the suffering many of those in our species endure throughout their whole lives. Why do certain cultures have little access to basic human rights and needs? Do these circumstances hold the power to separate people and cultures? Do human beings really care about the well-being of others?
Panama’s history is riddled by division between natives, colonizers, and expats. Within the tree-shaded islands of Bocas Del Toro lives a community of people who call themselves Ngäbe Buglé. Like many indigenous people today, they still face the impacts of European colonization. In 1996, Panamanian law created “la comarca Ngäbe Buglé”1 which is a reservation preserved specifically for the Ngäbe Buglé. Because of their isolated location and lack of transportation, the Ngäbe Buglé have little access to important services, such as healthcare.2 This is where their human rights are unmet: Article 29 of the United Nations Declaration on the Rights of Peoples states that
States shall also take effective measures to ensure, as needed, that programmes for monitoring, maintaining and restoring the health of peoples, as developed and implemented by the peoples affected by such materials, are duly implemented.3
If the states need to “take effective measures” to make sure that the indigenous peoples have health care, then why is access to healthcare one of the most pressing issues for the Ngäbe Buglé population? Indigenous communities everywhere struggle with access to the simple rights of living that are clearly stated within the United Nations Declaration on the Rights of Indigenous Peoples. Although these rights have been clearly outlined, there is no real strategy making it possible for these people to obtain those rights. McKenna Longacre, a student at Harvard Medical School, conducted a series of interviews in accordance with Floating Doctors, a nonprofit organization that provides healthcare popups in various communities who live in the Bocas Del Toro area of Panama, in which one local interviewee stated that the paucity of health care access is “a violation of human rights because [Panama] is not simply a resource poor country… there is actually enough money to make changes!”4 This conclusion further emulates the marginalization of indigenous peoples that dehumanizes them to the point that they are left out of basic human needs. After conducting her research project, Longacre concluded “the qualitative data suggested that lack of family planning has a direct and deleterious impact on local education, socioeconomic stability, and basic health of local communities.”5 Not only have these people been stripped of their basic human rights, but there is a significant need for reproductive health education and contraceptives: they have been in the midst of the detrimental results of overpopulation, poor family planning, and STD and STIs for years. What is even more disheartening is that these issues tend to affect young women more than anyone: “When you see children pregnant at 11 years old, it’s heartbreaking. It affects everything: status in the community, food, health… There is no aspect of health that is not affected by family planning.”6 In fact, young men and women who live in Comarcas tend to engage in sexual acts at a young age. Amanda Gabster, a doctoral student at the London School of Hygiene, conducted a study done within a population of people who live in comarca Ngäbe Buglé concluded that
26.1% of young women and 26.5% of young men reported to have engaged in sexual relations before the age of 15; among 15–24-year-olds, 4.8% of young women and 0.6% of young men reported having used a condom at sexual debut; and finally 81.2% adult and young women in the CNB [Comarca Ngäbe Buglé] report they cannot deny sexual relations with their partner (De Leon et al. 2018).7
It is a societal norm that condoms not be used, and even more shockingly, a large population of women feel as though they must engage in sexual activities with the person they are with. Consent is not a normalized concept in this indigenous population, and creates a snowball effect of STDs and unwanted pregnancies. While one of the best ways to prevent these accidental results of sexual intercourse is to use condoms and other forms of birth control, doing so is extremely difficult for populations who have little to no access to healthcare.
Unfortunately, many global communities struggle to hold any freedom. Whether it be the freedom to reproductive education and healthcare, or even the freedom to keep their land and their culture alive, it is a constant battle. The Ngäbe Buglé still face violence from people who want to take and exploit their natural resources. Paraiso For Sale, a documentary broadcast by PBS in 2011, shows the strife of the indigenous peoples who were enraged about their land being taken. One of the protesters passionately observes that “the lands of the indigenous are being commercialized by this government. They are opening the way for big investors. They are allowing them to snatch the best resources from the indigenous communities and farmers.”8 Such development runs directly counter to their rights as native people. Perhaps the insidious relationship between the government and the people of Panama creates tension between the indigenous peoples who want to conserve their land and culture, causing a dynamic in which people are afraid to seek healthcare because the ones who provide it are, to them, the same as those who have pushed them off their land throughout history. Meanwhile, the government fails to use its money for important resources, such as healthcare, and puts its funds into big companies, ignoring the voices of the indigenous peoples who constantly ask for better access to healthcare and living conditions. As a result, there is an endless cycle of fear and anger towards the government.
Once one understands how the Ngäbe Buglé’s land is being treated by the government, it is important to turn on the ways in which the government prevents family planning and the use of contraceptives. A report by the National Indigenous Women’s Cooperation of Panama brought together women from each of the seven indigenous groups in order for them to clarify their rights and to suggest changes to policies that cause issues for the women in these communities. The report describes several “barriers that limit [their] effective participation in the development of [their] communities”9 by blatantly calling out the lack of government policies that provide any sort of help for indigenous women. Not only is there a lack of governmental concern when it comes to healthcare, but there are more fundamental issues such as “racism, poverty, and lack of knowledge about sexuality within these communities’ world view”10 that lead to the high transmission rates of HIV, AIDS, and other STDs. On the topic of early pregnancies, they state that “there is no policy to raise awareness of this issue either within national or traditional government authorities.”11 Yes, government action is a huge factor when it comes to health care, but it goes beyond that. It is the history of the dehumanization and exploitation of indigenous peoples in the Americas that causes people to feel no remorse in the way they treat natives. Because western powers and those in charge of these countries have caused years of exploitation, they will continue to do it.
Exploitation manifests itself in different ways: the exploitation of a whole people and the exploitation of individuals. Sexual exploitation is largely a concern within communities where young girls are not educated on consent and other significant sexual health standards. The study by Amanda Gabster observes that “gender norms can indirectly affect the prevalence of STIs in several ways,” some of those ways being the “age of sexual debut or their decision to use a condom.”12 While it is clear that gender norms have an impact on sexual reproductive health, can the inverse occur? Does access to sexual reproductive healthcare have a large-scale impact on gender norms? A young indigenous girl stated that “Girls may be getting pregnant accidentally, but they don’t want to be pregnant.”13 If that is typically the case for these young women, the lack of sexual education can be reasonably deducted as a probable factor in the exceedingly high number of teenage pregnancies. In fact, an article published by the ACLU summarizing the impact of sexual education cited a study by the University of Washington that “found that adolescents who receive comprehensive sex education are significantly less likely to become pregnant than adolescents who receive abstinence-only-until-marriage or no formal sex education.”14 If the rate of teenage pregnancy has an inverse relationship with the lack of sexual education, then it is because of the lack of sexual resources, including education, that cause such high rates of pregnancy in the community of young Ngäbe Buglé women. A study done by Floating Doctors and Longacre that studied women between the ages of eighteen and fifty years old with more than two children found that “misconceptions about family planning and concerns about side effects are widespread and deter women from using family planning.”15
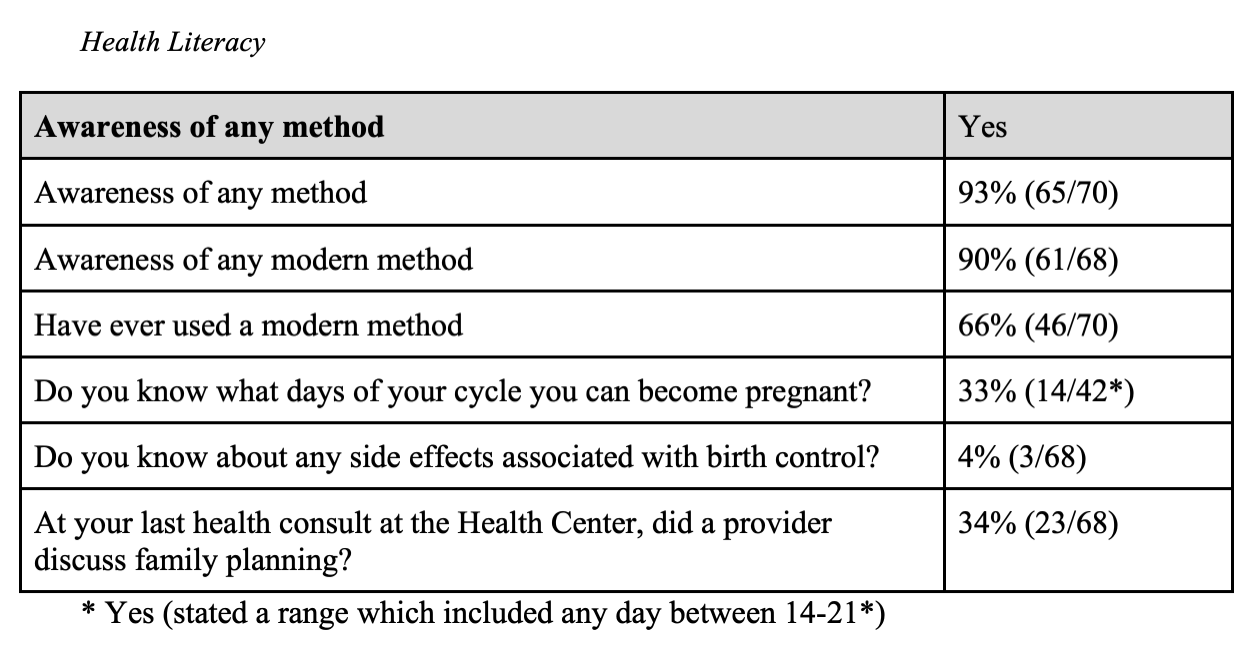
The figure above from Longacre’s study with the Floating Doctors shows that the percentages of the people who answered specific questions about their relationship to methods and knowledge of birth control. It concludes that there is an “unmet need”17 for methods of contraception. Yet another variable stands out: only 34% of people had any sort of consultation about family planning. If the government does not provide adequate healthcare resources, then who will?
Floating Doctors distributes condoms and a form of birth control called “Depo.” This shot is injected into a woman’s arm, and prevents pregnancy for three months. It stops ovulation, and creates an extra layer of mucus around the cervix.18 Although effective, it does not last long, and it can lead to other negative health problems that its users will most likely not be able to get treated. In the face of these uncommon risks, any access to birth control will decrease the high percentage of unwanted pregnancies within the community of young women in the Ngäbe Buglé tribe. Not only does Floating Doctors have the potential to provide adequate reproductive resources, but “the number of annual patient encounters has increased from 3,000 at the time of the original study, to now over 11,000 per year.”19 This statistic was published in 2017, so one can imagine an even larger expansion of these services since then and in years to come. With no real progress from government funded healthcare for indigenous peoples in Panama, the Floating Doctors are the best bet for these people to be treated by professionals and to be treated as human beings.
The complicated relationship between non-native and native people continues to be a barrier, but even the indigenous people acknowledge the importance of family planning and reproductive health in their community. A community member stated that “family planning is the biggest problem of human rights.”20 If family planning is such an important human rights issue to which these people do not have real access, then Article 29 of the United Nations Declaration on the Rights of Indigenous Peoples fails at its purpose. But how much should indigenous communities in Panama really rely on a document written by non-Panamanians anyway? Through various connections and conversations with the Ngäbe Buglé people, there is a common thread that refers to the failure to protect human rights, and has led to a paucity in reproductive healthcare access, directly affecting the wellbeing and gender dynamics of the Ngäbe Buglé tribe.
Bright, Marshall. “Study Finds That Comprehensive Sex Education Reduces Teen Pregnancy.” American Civil Liberties Union. American Civil Liberties Union, February 17, 2012. https://www.aclu.org/news/reproductive-freedom/study-finds-comprehensive-sex-education-reduces-teen-pregnancy.
Few for Change. “An Overview of Panama’s Communities: Part I – Western Panama.” Few for Change, November 5, 2020. https://www.fewforchange.org/blog/2020/7/an-overview-of-panamas–communities-part-i.
Gabster, Amanda, Philippe Mayaud, Juan Miguel Pascale, and Beniamino Cislaghi. “Gender Norms and Sexual Behaviours among Youth of the Comarca Ngäbe-Buglé, Panama.” Culture, health & sexuality. U.S. National Library of Medicine, September 2020. https://www.ncbi.nlm.nih.gov/pubmed/31429382.
Informe: Las gestiones de delimitación de la comarca indígena ngöbe buglé: 1982-1996 (1996).
“Is Depo-Provera Safe?: See If Depo-Provera Is Right for You.” Planned Parenthood. Accessed April 13, 2022. https://www.plannedparenthood.org/learn/birth-control/birth-control-shot/how-safe-is-the-birth-control-shot.
Longacre, Mckenna Mary. “A Needs Assessment of Family Planning within a Ngöbe–Buglé Patient Population in Bocas Del Toro, Panama.” DASH Home, January 1, 1970. https://dash.harvard.edu/handle/1/32676115.
“Paraiso for Sale.” impacto films, 2011. http://www.impactofilms.com/paraiso-for-sale.html.
“Tbinternet.ohchr.org.” The VOICE of Panama’s Women, November 27, 2009. https://tbinternet.ohchr.org/Treaties/CEDAW/Shared%20Documents/PAN/INT_CEDAW_NGO_PAN_45_9855_E.pdf.
“United Nations Declaration on the Rights of Peoples for Peoples.” United Nations. United Nations. Accessed April 13, 2022. https://www.un.org/development/desa/peoples/declaration-on-the-rights-of–peoples.html.
1. “Informe: Las Gestiones De delimitación De La Comarca indígena ngöbe buglé: 1982-1996,” Informe: Las gestiones de delimitación de la comarca indígena ngöbe buglé: 1982-1996 § (1996), 1.
2. Few for Change, “An Overview of Panama’s Communities: Part I – Western Panama,” Few for Change (Few for Change, November 5, 2020), https://www.fewforchange.org/blog/2020/7/an-overview-of-panamas–communities-part-i.
3. “United Nations Declaration on the Rights of Peoples for Peoples,” United Nations (United Nations, 2017), https://www.un.org/development/desa/peoples/declaration-on-the-rights-of–peoples.html.
4. Mckenna Mary Longacre, “A Needs Assessment of Family Planning within a Ngöbe–Buglé Patient Population in Bocas Del Toro, Panama,” DASH Home, January 1, 1970, https://dash.harvard.edu/handle/1/32676115, 38.
5. Longacre, 44.
6. Longacre, 58.
7. Amanda Gabster et al., “Gender Norms and Sexual Behaviours among Youth of the Comarca Ngäbe-Buglé, Panama,” Culture, Health & Sexuality 22, no. 9 (2019): pp. 1033, https://doi.org/10.1080/13691058.2019.1648873.
8. “Paraiso for Sale,” impacto films, 2011, http://www.impactofilms.com/paraiso-for-sale.html.
9. “Tbinternet.ohchr.org” (The VOICE of Panama’s Women, November 27, 2009), https://tbinternet.ohchr.org/Treaties/CEDAW/Shared%20Documents/PAN/INT_CEDAW_NGO_PAN_45_9855_E.pdf, 1.
10. The VOICE of Panama’s Women, 2.
11. The VOICE of Panama’s Women, 2.
12. Amanda Gabster, 1033.
13. Amanda Gabster, 1033.
14. Marshall Bright, “Study Finds That Comprehensive Sex Education Reduces Teen Pregnancy,” American Civil Liberties Union (American Civil Liberties Union, February 17, 2012), https://www.aclu.org/news/reproductive-freedom/study-finds-comprehensive-sex-education-reduces-teen-pregnancy
15. Longacre, 46.
16. Longacre, 54.
17. Longacre, 31.
18. “Is Depo-Provera Safe?: See If Depo-Provera Is Right for You,” Planned Parenthood, accessed March 31, 2022, https://www.plannedparenthood.org/learn/birth-control/birth-control-shot/how-safe-is-the-birth-control-shot.
19. Longacre, 49.
20. Longacre, 57.
 16
16